
What is Shoulder Dystocia? It's a very rare and serious complication in which baby's shoulders get stuck that affects babies of all sizes, though it occurs slightly more frequently in babies that are over 9lbs. It's still rare, however, and not something that you should spend time worrying about. There is no way to accurately predict it ahead of time and any provider talking about it is likely looking for the bigger paycheck that comes with a cesarean birth (the difference? vaginal birth: $10K, cesarean birth: $25K and a VBAC costs more than a regular vaginal birth, thus, it's always in an OBs best financial interest to go for a cesarean--though it's NOT in mom's OR baby's, as mom is 5.5 times more likely to die and baby is 3 times more likely to die and complications of less serious natures are far more frequent as well).
So, doctors love to say, "Your baby is too big," (usually based on faulty ultrasound data, despite the fact that ultrasounds can be wrong by 2lbs or even more and become useless in determining size after week 20). The reason is usually shoulder dystocia. Many techniques have been used over the years, including just killing the baby, though the most success has been found in the easiest technique to date--the Gaskin Maneuver. The Gaskin Maneuver consists of having mom roll onto all fours (or assisting if necessary). During the process, many babies become dislodged and pop right out. If this doesn't happen, then the doctor actually has better access to help wiggle the baby around until the shoulder releases and the rest of baby is born (Woods or Rubin maneuver).
Most obstetricians don't even know that this maneuver exists, though most midwives are trained in it. In one study, it was shown to be effective in 83% of use without any further maneuvers. No maternal or perinatal mortality occurred. Morbidity was noted in only four deliveries: a single case of postpartum hemorrhage that did not require transfusion (maternal morbidity, 1.2%), one infant with a fractured humerus and three with low APGAR scores (neonatal morbidity, 4.9%).
Many doctors use traction (pulling on baby's head) or fundal pressure (where the nurse climbs on the bed and jumps down onto your stomach) before anything else and these are not only the least effective techniques, but dangerous to mother and baby.
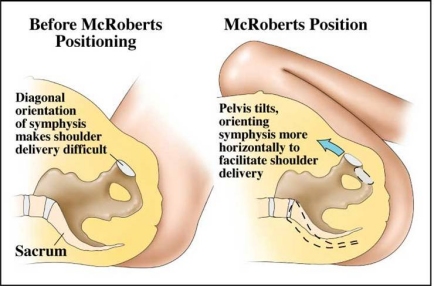
The McRoberts maneuver (where mom's legs are brought up as far back toward her stomach as possible, which realigns the pubic bone and can slip baby's shoulder out) should be tried first and if failing, suprapubic pressure (where the doctor or nurse makes a fist and pushes hard on the baby's shoulder just above the pubic bone) can be applied. Next, the Gaskin maneuver should be performed and if that fails, then Woods and Rubin maneuvers can be tried.
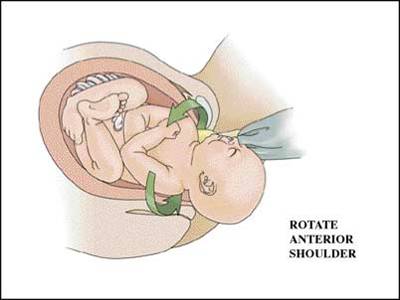
McRoberts is effective in 39.5% of cases and in 58% with the addition of the suprapubic pressure. These methods can cause serious injury to the mother (McRoberts can injure mom's legs, particularly the femur and hips), but are typically safe to the baby. Woods does not have an available statistic for effectiveness and can break the baby's humerus. The Rubin maneuver is the opposite of Woods and requires less traction and causes significantly less injury.
Australia is currently training doctors in fracture of the clavicle, which has been dismissed until now as so dangerous to the baby and difficult to perform that it should not be used. However, it is used in some cases and can be lifesaving for baby. It's a severe emergency procedure that should not be attempted until all others have failed.
The Gaskin maneuver is most criticized due to it requiring the mother to be able to roll over and support herself on her hands and knees--something that is difficult, if not impossible, to do with a normal epidural. That's the only criticism, however, that is keeping it from being more widely studied and implemented.
The evidence from the literature on shoulder dystocia shows clearly that shoulder dystocia cannot be predicted with any degree of accuracy and it cannot be prevented by any specific strategies or maneuvers. Half of the babies in the Gaskin study were not larger than average and many were in the 5lb range. The worst outcomes did occur in the 'macrosomic' (larger than 10lbs) category. However, 'macrosmia' is not a sole cause nor does it always lead to shoulder dystocia. In fact, over 90% of macrosomic babies can be delivered vaginally without incident.
Perhaps in those "birth plan creators" that are available all over the internet that include sections on emergency births, preferences on maneuvers should be included in the event of shoulder dystocia. It's unlikely that doctors would be open to this, however, despite evidence of effectiveness and safety of the procedure, simply because they have no experience with it.
The best thing you can do as a pregnant woman is to be educated and if your doctor brings up the issue, discuss it with him/her. Eve if they don't, it might be useful to know their typical management of shoulder dystocia in case of emergency and their willingness to attempt maneuvers with less risk to mother and baby, even if unconventional, before the more dangerous, riskier maneuvers. It's also important to stay calm and follow your care provider's direction if the complication does arise.
Maneuver illustrations:
Traction:
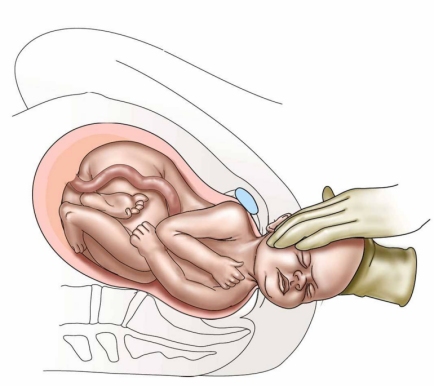
McRoberts:
suprapubic pressure:

Woods Screw Maneuver:
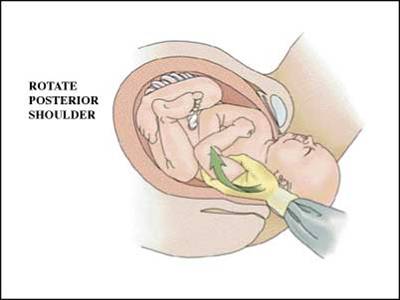
Rubin Maneuver:
Gaskin Maneuver:

This and your previous post are both such excellent resources! Thank you for writing them!
ReplyDelete