For all intents and purposes, this blog refers to Type A1 gestational diabetes only: "abnormal oral glucose tolerance test (OGTT) but normal blood glucose levels during fasting and 2 hours after meals; diet modification is sufficient to control glucose levels"1
So, you're in the sixth month of pregnancy and the doctor says that at your next appointment, you are going to be tested for gestational diabetes. She explains that you are going to be given a drink an hour before blood is drawn to see if you have GD. She doesn't give you much other information. At some offices, you will be sent home with the glucola (sometimes you even get to pick your flavor), while at others, you go in the day of testing, an hour before, and are given the drink.
Let's say you're in the second group, like I was the first time. So, on the day of, you get up and have breakfast as usual. A couple hours later, you go in and you get your drink. You choke it down (I thought it tasted fine, but many women complain of the taste) and then go sit in the chairs to wait for your test. You go to the phlebotomist's chair and she either draws a vial of blood or pricks your finger, depending on the office. You get your bandaid and go home (probably craving something high in protein or a lot of water).
You go in for your next appointment to find out you failed the test. Next, you are told that you'll have to take the fasting three hour test. You are given a date and you fret and worry about what this means. Your doctor assures you that many women who fail the one hour test pass the three hour test.
So, on the day of, you go in, your stomach growling, possibly having a return of the dreaded morning sickness because your blood sugar is so low. They take your blood and send you off with your drink. You choke it down (it's even worse this time) and are informed that if you throw up or consume anything else, you automatically fail and have to do it again. You can have as much water as you want, though.
You go sit in the chairs and read a book or magazine for the next hour, or watch a movie on a portable DVD player. You get your blood taken again. Then back to the chairs. At this point, you may be feeling dizzy and faint. You reach your chair gratefully and try hard to distract yourself against how crummy you're feeling. The second hour takes forever to pass, but you get there and have your blood drawn again. At this point, you may feel irritable and nauseated. You don't want to do this again, though, so you desperately try to
not throw up. Just one more hour. Maybe you have some water. You probably need to pee. The baby's hyper and the rolling around and elbowing you in the stomach is not helping your nausea. You pick up your book or movie and put it down, unable to concentrate. You space off. You finally get back to reading or watching and find out that you made it. One last poke and the vampire is done with you.
You bolt from the office right for the nearest fast food to appease the baby, who is sucking all the nutrients from your starved body. Food at last!! You find out at the follow up appointment that you failed. You're told your numbers: 80, 195, 156, 120. These numbers probably don't mean a lot to you, especially since you're devastated and wondering what this all means to you. No more crackers in the morning? No cake at your baby shower?
You're told that you just need to monitor your sugar and diet and see a nutritionist and that there is no reason to worry. You are now high risk and will probably have a huge baby who will need bottles to stabilize him after he's born, but it's okay. The doctor will perform a cesarean to save you from this all if she needs to. You should probably try to pump some milk to prepare if you don't want the hospital to give your baby a bottle.
Now, let's examine what you should have questioned in the above scenario.
"...you get up and have breakfast as usual."
The day of your one hour test, you should be careful about your breakfast. Avoid carbohydrates as much as you can--absolutely no juice or soda pop! If you drink coffee, it should be black. If you drink tea, the same thing. The absolute best thing for you is to only drink water. Even milk is full of sugar. No bananas! They may seem like an innocent fruit, but they are a sugar-spiking fiend in the least diabetic of people! Have some eggs and bacon. Not the healthiest breakfast, no, but you need protein to break down blood sugar in your body. Have a handful of raw almonds, too (or any natural nut of your choice).
"You go sit in the chairs and read a book or magazine for the next hour, or watch a movie on a portable DVD player."
Don't sit! If you have a long drive to the doctor after drinking your glucola, then go an hour early and drink it there. Walk around the office. Jog. Do some light exercise that you would normally do. But whatever you do, don't just sit there. Your body won't burn the carbs properly just by sitting. Don't worry about what other people think about it, lead by example or at least just protect your own body.
If you fail the one hour test still, there isn't a lot you can do for the three hour test, except to remain active throughout, no matter how crappy you feel. You can avoid a lot of carbs the day before it, but you need to keep your blood sugar as level as possible.
Next, know your numbers! The list of numbers I gave before indicates someone who does
not have diabetes. In fact, they were almost exactly my numbers. The first is a normal fasting glucose number, then the second is a high spike that isn't an abnormal reaction to the amount of glucola that they give you. The third is one point above fail, which is a faster sugar drop than they are looking for, but they look solely at numbers, not at pattern. The final number is more than just a passing number--it's a pass with flying colors. Again, this pattern should be seen as a sign of insulin working pretty well, but it's a definite fail. If the numbers had looked like this:
95, 200, 165, 145
Then you most definitely have a problem.
Now, it's not a bad thing to follow a healthy diabetic diet with a failed test and to monitor your sugar, particularly if you've had symptoms (extreme thirst, dizziness, nausea) to identify problem areas. Me, I found out that I was waking up borderline hypoglycemic (70mg/dl) if I didn't have a chocolate cake at bedtime each night. Yes, Little Debbie and I had a standing appointment. She didn't spike me and I didn't feel like crap when I woke up in the morning. Win-win. Medicinal chocolate, lol.
Now, where it
is dangerous is the assumption that any level of glucose intolerance (including just being intolerant to the stupid test) will negatively impact the baby. Let's start with "big baby".
First, as recently as the early 1900s, a 10lb baby received congratulations to the mother for growing such a 'healthy baby' and a 6lb baby was received in hushed tones and worries about such a small baby being born. Sometimes the mother was even scolded for 'starving' her baby (even though 6lbs is a valid weight, as is 10lbs). Now, the average is 7.5lbs, but that's hardly a cutoff. After all, women can birth nearly 14lb babies naturally.2 Many women that I've known report that their bigger, 9-11lb babies were actually easier than their smaller (6-8lb) ones! Not always, of course--my best friend's mom had problems with her nearly 12lb baby in that she tore six ways to Sunday, but her others were 11-something, 10-something and a couple of 9lbers and she didn't have problems.
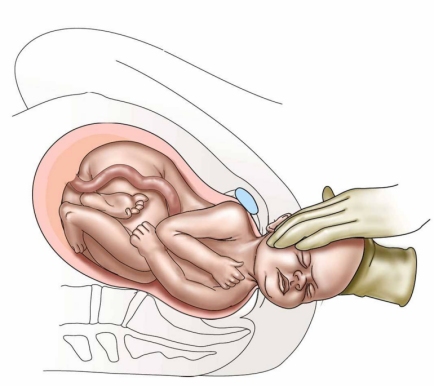
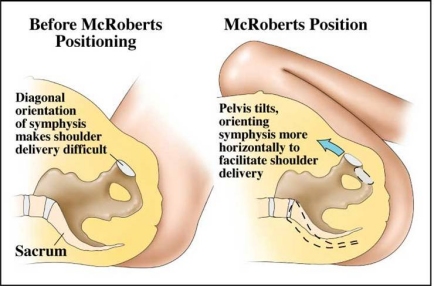
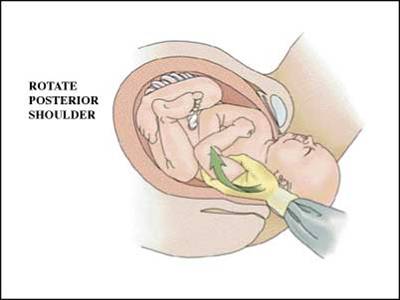
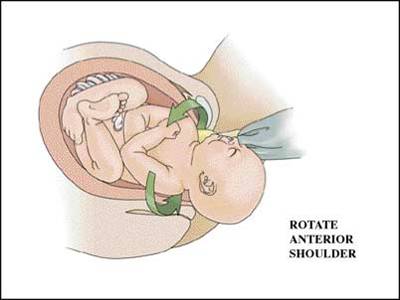
A lot of the worry about big babies comes from shoulder dystocia. This is a very rare complication that can occur in babies of any size, but is considered higher risk in babies of larger sizes. The true risks of shoulder dystocia include: malpositioned baby, mother in the lithotomy position or otherwise on her back and/or tailbone and any monitoring or drugs that limit mother's movement (if you're going to get an epidural, make sure it's the lowest dose they can do or that it's turned off long before pushing!). If you suspect a large baby, it's important to have a provider who knows the Gaskin Maneuver,3 which has been shown quite successful and is pretty easy--just roll mom onto all fours. From that position, if baby is not released by the act of rolling over, some otherwise difficult maneuvers become much easier to perform to attempt to dislodge baby. If unsuccessful, mom can be rolled back and the usual "nurse jumps on the fundus" maneuver that most OBs use exclusively, can be performed. This is very dangerous for the baby, so it should be left as a last resort. However, a cesarean is not needed in most cases and never to just prevent the possibility of a rare incidence.
If you're worried about a big baby and tearing--let me tell you, as someone who's had both a cesarean and a terrible, messy tear with my VBAC, that a tear is preferable to recovering from abdominal surgery. Especially with a dependent infant!
The next risk for a baby in regards to gestational diabetes is elevated blood sugar leading to crash at birth. If mom's sugars are well-regulated, this isn't actually a risk. Some researchers believe that much of the elevated sugar accompanied by no symptoms is actually natural stores in the maternal bloodstream as backup for the baby and doesn't actually
go to the baby.4 However, in cases of controlled sugars, there is no excess to cause the spike that leads to the crash and it's more likely that the fasting during labor may be a bigger risk to the baby (eat during labor, ladies, regardless of 'hospital policy' or diabetes status! It matters!), leaving baby born with low blood sugar. Bring baby straight to breast from birth to help with this.
The real risk of being diagnosed with gestational diabetes is that your chances of cesarean skyrocket because management may lead to risk factors for pre-eclampsia. Also, many women are not properly counseled or are told to "avoid carbs" (very dangerous for both mom and baby! Diabetics take in more carbs than you are probably aware!) or go straight on insulin (also dangerous, as taking insulin with no need can lead to an insulin coma).
So, before you just blindly consent to the test, ask your doctor or midwife what options are available. If you are in a low risk category, request being allowed to skip. If you cannot, ask what other forms of testing are available that would be easier on your body and your baby if you fail the one hour test (and do
not consent to the fasting one hour test--it's outdated). Find out how your practitioner will respond if you fail the tests and if they start talking about cesareans--get another doctor. I still, to this day, regret not following that advice. Also find out hospital policy as to what they will do to your baby, particularly if you plan on breastfeeding.
In the end, non-insulin-dependent gestational diabetes is really not a cause for concern--at least not regarding birth. Don't freak out and don't let yourself be 'managed' into unnecessary surgery.
Like many women, after I was diagnosed with gestational diabetes, I never showed any symptoms and my sugar never spiked into the danger zone. The worst it got was after my baby shower, where I had ice cream cake, fruit pizza and bread rolls. It was no higher than expected in a non-diabetic after
that fair, either! My baby was the exact same weight at 42 weeks as her sister at 39weeks, 6 days (who I did not have GD with).
Knowing this is important as well to know that not all women diagnosed with GD are at risk for Type 2 diabetes, despite the media hype to the contrary.
If you'd like to avoid the risk altogether, you might consider
Dr. Brewer's Diet which is available for many dietary needs.
1.Gabbe S.G., Niebyl J.R., Simpson J.L. OBSTETRICS: Normal and Problem Pregnancies. Fourth edition. Churchill Livingstone, New York, 2002
2. CTV News: B.C. Family Welcomes Very Big Bundle of Joy
3. The Gaskin Maneuver and The Farm Midwives: Dystocia
4. "Gestational Diabetes: Myth or Metabolism?" by Joy Jones, RN (p. 59)